
Fibromyalgia
Definition of Fibromyalgia
Fibromyalgia (FM or FMS) is characterised by chronic widespread pain and allodynia (a heightened and painful response to pressure). Its exact cause is unknown but is believed to involve psychological, genetic, neurobiological and environmental factors. Fibromyalgia symptoms are not restricted to pain, leading to the use of the alternative term fibromyalgia syndrome for the condition. Other symptoms include debilitating fatigue, sleep disturbance, and joint stiffness. Some patients also report difficulty with swallowing, bowel and bladder abnormalities, numbness and tingling, and cognitive dysfunction Fibromyalgia is frequently comorbid with psychiatric conditions such as depression and anxiety and stress-related disorders such as posttraumatic stress disorder. Not all fibromyalgia patients experience all associated symptoms.
There is evidence that environmental factors and certain genes increase the risk of developing fibromyalgia – these same genes are also associated with other functional somatic syndromes and major depressive disorder. The central symptom of fibromyalgia, namely widespread pain appears to result from neuro-chemical imbalances including activation of inflammatory pathways in the brain which results in abnormalities in pain processing. The brains of fibromyalgia patients show functional and structural differences from those of healthy individuals, but it is unclear whether the brain anomalies cause fibromyalgia symptoms or are the product of an unknown underlying common cause. Some research suggests that these brain anomalies may be the result of childhood stress, or prolonged or severe stress.
Causes of Fibromyalgia
The cause of fibromyalgia is unknown. However, several hypotheses have been developed including “central sensitization”. This theory proposes that fibromyalgia patients have a lower threshold for pain because of increased reactivity of pain-sensitive nerve cells in the spinal cord or brain. Neuropathic pain and major depressive disorder often co-occur with fibromyalgia – the reason for this comorbidity appears to be due to shared genetic abnormalities, which leads to impairments in monoaminergic, glutamatergic, neurotrophic, opioid and proinflammatory cytokine signaling. In these vulnerable individuals psychological stress or illness can cause abnormalities in inflammatory and stress pathways which regulate mood and pain. Eventually a sensitisation and kindling effect occurs in certain neurones leading to the establishment of fibromyalgia and sometimes a mood disorder. The evidence suggests that the pain in fibromyalgia results primarily from pain processing pathways functioning abnormally.
In simple terms it can be described as the volume of the neurones being set too high and this hyper-excitability of pain processing pathways and under-activity of inhibitory pain pathways in the brain results in the affected individual experiencing pain. Some of the neurochemical abnormalities that occur in fibromyalgia also regulate mood, sleep and energy, thus explaining why mood, sleep and fatigue problems are commonly co-morbid with fibromyalgia.
Signs and Symptoms of Fibromyalgia
 The defining symptoms of fibromyalgia are chronic widespread pain, fatigue, sleep disturbance, and heightened pain in response to tactile pressure (allodynia).
The defining symptoms of fibromyalgia are chronic widespread pain, fatigue, sleep disturbance, and heightened pain in response to tactile pressure (allodynia).
Other symptoms may include tingling of the skin (paresthesias), prolonged muscle spasms, weakness in the limbs, nerve pain, muscle twitching, palpitations, and functional bowel disturbances.
Many patients experience cognitive dysfunction (known as “fibrofog”), which may be characterized by impaired concentration, problems with short and long-term memory, short-term memory consolidation, impaired speed of performance, inability to multi-task, cognitive overload, and diminished attention span. Fibromyalgia is often associated with anxiety and depressive symptoms.
Other symptoms often attributed to fibromyalgia that may possibly be due to a comorbid disorder include myofascial pain syndrome, also referred to as chronic myofascial pain, diffuse non-dermatomal paresthesias, functional bowel disturbances and irritable bowel syndrome, genitourinary symptoms and interstitial cystitis, dermatological disorders, headaches, myoclonic twitches, and symptomatic hypoglycemia. Although fibromyalgia is classified based on the presence of chronic widespread pain, pain may also be localized in areas such as the shoulders, neck, low back, hips, or other areas. Many sufferers also experience varying degrees of myofascial pain and have high rates of comorbid temporomandibular joint dysfunction. 20–30% of patients with rheumatoid arthritis and systemic lupus erythematosus may also have fibromyalgia.
Risk Factors for Fibromyalgia
Genetics
The mode of inheritance is currently unknown, but it is most probably polygenic. Research has also demonstrated that fibromyalgia is potentially associated with polymorphisms of genes in the serotoninergic, dopaminergic and catecholaminergic systems. However, these polymorphisms are not specific for fibromyalgia and are associated with a variety of allied disorders (e.g. chronic fatigue syndrome, irritable bowel syndrome) and with depression. Individuals with the 5-HT2A receptor 102T/C polymorphism have been found to be at increased risk of developing fibromyalgia.
Lifestyle
Stress may be an important precipitating factor in the development of fibromyalgia. Fibromyalgia is frequently comorbid with stress-related disorders such as chronic fatigue syndrome, posttraumatic stress disorder, irritable bowel syndrome and depression. A systematic review found significant association between fibromyalgia and physical and sexual abuse in both childhood and adulthood, although the quality of studies was poor. Poor lifestyles including being a smoker, obesity and lack of physical activity may increase the risk of an individual developing fibromyalgia.
Two studies that employed single-voxel magnetic resonance spectroscopy (1H-MRS) reported metabolic abnormalities within the hippocampal complex in patients with fibromyalgia. As the hippocampus plays crucial roles in maintenance of cognitive functions, sleep regulation, and pain perception, it was suggested that metabolic dysfunction of the hippocampus may be implicated in the appearance of these symptoms.
Some authors have proposed that, because exposure to stressful conditions can alter the function of the hypothalamic-pituitary-adrenal (HPA) axis, the development of fibromyalgia may stem from stress-induced disruption of the HPA axis.
Sleep disturbances
In 1975, Moldofsky and colleagues reported the presence of anomalous alpha wave activity (typically associated with arousal states) measured by electroencephalogram (EEG) during non-rapid eye movement sleep of “fibrositis syndrome” patients. By disrupting stage IV sleep consistently in young, healthy subjects, the researchers reproduced a significant increase in muscle tenderness similar to that experienced in “neurasthenic musculoskeletal pain syndrome” but which resolved when the subjects were able to resume their normal sleep patterns. In one study it was found that the best predictor of the experience of pain in male fibromyalgia patients was sleep quality.
Psychological factors
There is strong evidence that major depression is associated with fibromyalgia (1999), although the nature of the association is debated. A comprehensive review into the relationship between fibromyalgia and major depressive disorder (MDD) found substantial similarities in neuroendocrine abnormalities, psychological characteristics, physical symptoms and treatments between fibromyalgia and MDD, but currently available findings do not support the assumption that MDD and fibromyalgia refer to the same underlying construct or can be seen as subsidiaries of one disease concept. Indeed, the sensation of pain has at least two dimensions: a sensory dimension which processes the magnitude and location of the pain, and an affective-motivational dimension which processes the unpleasantness. Accordingly, a study that employed functional magnetic resonance imaging to evaluate brain responses to experimental pain among fibromyalgia patients found that depressive symptoms were associated with the magnitude of clinically induced pain response specifically in areas of the brain that participate in affective pain processing, but not in areas involved in sensory processing which indicates that the amplification of the sensory dimension of pain in fibromyalgia occurs independently of mood or emotional processes.
Physical trauma
Neck trauma has been reported to increase the risk of developing fibromyalgia.
Small bowel bacterial overgrowth syndrome
In a small 2004 double-blind study, all of the 42 FMS patients were found to have raised hydrogen levels in a lactulose hydrogen breath test, thought to indicate the presence of small bowel bacterial overgrowth syndrome. It has been hypothesised that chronic activation of the immune system against pathogenic bacterial overgrowth may cause fibromyalgia symptoms.
Diagnosis of Fibromyalgia
There is no single test that can fully diagnose fibromyalgia and there is debate over what should be considered essential diagnostic criteria and whether an objective diagnosis is possible. In most cases, patients with fibromyalgia symptoms may also have laboratory test results that appear normal and many of their symptoms may mimic those of other rheumatic conditions such as arthritis or osteoporosis. In general, most doctors diagnose patients with a process called differential diagnosis, which means that doctors consider all of the possible things that might be wrong with the patient based on the patient’s symptoms, gender, age, geographic location, medical history and other factors. They then narrow down the diagnosis to the most likely one. The most widely accepted set of classification criteria for research purposes was elaborated in 1990 by the Multicenter Criteria Committee of the American College of Rheumatology. These criteria, which are known informally as “the ACR 1990″, define fibromyalgia according to the presence of the following criteria:
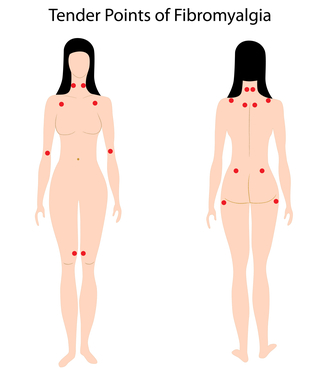
A history of widespread pain lasting more than three months—affecting all four quadrants of the body, i.e., both sides, and above and below the waist.
Tender points—there are 18 designated possible tender points (although a person with the disorder may feel pain in other areas as well). Diagnosis is no longer based on the number of tender points.
The ACR criteria for classification of patients were originally established as inclusion criteria for research purposes and were not intended for clinical diagnosis but have now become the de facto diagnostic criteria in the clinical setting. It should be noted that the number of tender points that may be active at any one time may vary with time and circumstance. A controversial study done by a legal team looking to prove their client’s disability based primarily on tender points and their widespread presence in non-litigious communities prompted the lead author of the ACR criteria to now question the useful validity of tender points in diagnosis.
Use of control points has been used to cast doubt on whether a person has fibromyalgia, and to claim the person is malingering, however, no research has been done for the use of control points to diagnose fibromyalgia and such diagnostic tests have been advised against and that patients complaining of pain all over should still have fibromyalgia considered as a diagnosis. Since the ACR criteria were originally published, research with mechanical devices that exert defined pressure indicate that diagnosis of fibromyalgia cannot be done objectively by machine and require a physician’s subjective estimate of how much pressure should be exerted.
Fibromyalgia is widely under-diagnosed with up to 75 percent of people suffering with fibromyalgia not being diagnosed.
Prevention from Fibromyalgia
- Fibromyalgia can’t be prevented by the risk factors can be reduced with these methods:
- Reduce stress with management techniques
- Get sufficient sleep
- Exercise regularly
- Eat healthy foods and limit caffeine intake
- Pace yourself
Treatment of Fibromyalgia
As with many other medically unexplained syndromes, there is no universally accepted treatment or cure for fibromyalgia, and treatment typically consists of symptom management. Developments in the understanding of the pathophysiology of the disorder have led to improvements in treatment, which include prescription medication, behavioral intervention and exercise. Indeed, integrated treatment plans that incorporate medication, patient education, aerobic exercise and cognitive-behavioral therapy have been shown to be effective in alleviating pain and other fibromyalgia-related symptoms.
Psychological therapies
Cognitive behavioural therapy (CBT) and related psychological and behavioral therapies have a small to moderate effect in reducing symptoms of fibromyalgia. The greatest benefit occurs when CBT is used along with exercise.
CBT improves self-efficacy or coping with pain and reduces the number of physician visits at post-treatment, but has no significant effect on pain, fatigue, sleep or health related quality of life at post-treatment or followup. Depressed mood was also improved but this could not be distinguished from some risks of bias. A multidisciplinary approach, often including CBT is sometimes considered to be the “gold standard” of treatment for chronic pain syndromes such as fibromyalgia.
Medications
Health Canada and the US Food and Drug Administration (FDA) have approved pregabalin and duloxetine, for the management of fibromyalgia. The FDA also approves milnacipran, but the European Medicines Agency refused marketing authority.
Antidepressants
Antidepressants are “associated with improvements in pain, depression, fatigue, sleep disturbances, and health-related quality of life in patients with FMS.” The goal of antidepressants should be symptom reduction and if used long term, their effects should be evaluated against side effects. A small number of people benefit significantly from the SNRIs duloxetine and milnacipran and the tricyclic antidepressants (such as amitriptyline) however many people experience more adverse effects than benefits. While amitriptyline has been used as a first line treatment, the quality of evidence to support this use is poor.
Anti-seizure medication
The anti-convulsant drugs gabapentin and pregabalin may be used. Gabapentin is of a significant benefit in about 30% of people who take it however is commonly associated with adverse effects. A Cochrane review of pregabalin use in chronic pain concluded that “A minority of patients will have substantial benefit with pregabalin, and more will have moderate benefit. Many will have no or trivial benefit, or will discontinue because of adverse events.” A meta-analysis of four trials of pregabalin in fibromyalgia found that, for people who did respond to pregabalin, there was a reduction in their time off work of greater than 1 day per week.
Opioids
The combination of tramadol and paracetemol has demonstrated efficacy, safety and tolerability (for up to two years in the management of other pain conditions) without the development of tolerance. It is as effective as a combination of codeine (another mild opioid) and paracetamol but produces less sleepiness and constipation.
Others
The narcolepsy medication sodium oxybate has been studied in those with fibromyalgia. This drug was shown to reduce the symptoms of pain and fatigue, and dramatically reduce the sleep abnormalities (alpha intrusion and decreased slow-wave sleep). Subsequent stage 3 trials for this drug supported these findings which found the drug provided important benefits across multiple symptoms in subjects with fibromyalgia. Since Sodium Oxybate was shown to increase natural growth hormone production levels through increased slow-wave sleep patterns, these studies provide further support that supplementing growth hormone may be beneficial for fibromyalgia sufferers. However, this medication was not approved by the FDA for the indication for use in fibromyalgia patients due to the concern for abuse.
The muscle relaxants cyclobenzaprine and tizanidine are sometimes used off-label to treat fibromyalgia. A small clinical trial of very low doses of cyclobenzaprine taken between dinner and bedtime demonstrated improved musculoskeletal pain, fatigue, tenderness and depressed symptoms in FM patients, as well as an improvement in objective measures of sleep quality.
Dopamine agonists (e.g. pramipexole (Mirapex) and ropinirole (ReQuip)) resulted in some improvement in a minority of patients, but numerous side effects, including the onset of impulse control disorders like compulsive gambling and shopping, have led to concern about this approach.
The use of NSAIDs is not recommended as first line therapy. It can take up to three months to derive benefit from the antidepressant amitriptyline and up to six months to gain maximal response from duloxetine, milnacipran, and pregabalin. Some medications have the potential to cause withdrawal symptoms when stopping so gradual discontinuation may be warranted particularly for antidepressants and pregabalin.
Evidence exists that fibromyalgia is a neuro-immuno-endocrine disorder. Elevations in substance P, IL-6 and IL-8 as well as corticotropin-releasing hormone have been found in the cerebral spinal fluid of fibromyalgia suffering individuals. Increased numbers of mast cell numbers have been found in skin biopsies of some individuals with fibromyalgia. Quercetin, a pharmacologically active natural product which possesses anti-inflammatory in addition to mast cell inhibiting properties may be a useful treatment.
Exercise
Exercise improves fitness and sleep and may reduce pain and fatigue in some people with fibromyalgia. In particular, there is strong evidence that cardiovascular exercise is effective for some patients. Long-term aquatic-based exercise has been proven beneficial as it combines cardiovascular exercise with resistance training. However, due to the cold sensitivities of people with fibromyalgia syndrome, aquatic therapy must take place in a warm pool. Not only that, but the air temperature outside of the pool must also be heated to prevent fibromyalgia patients from getting chills and aches when out of the water. This involves a specialised pool facility, which makes this therapy more expensive and less accessible than regular swimming exercise.